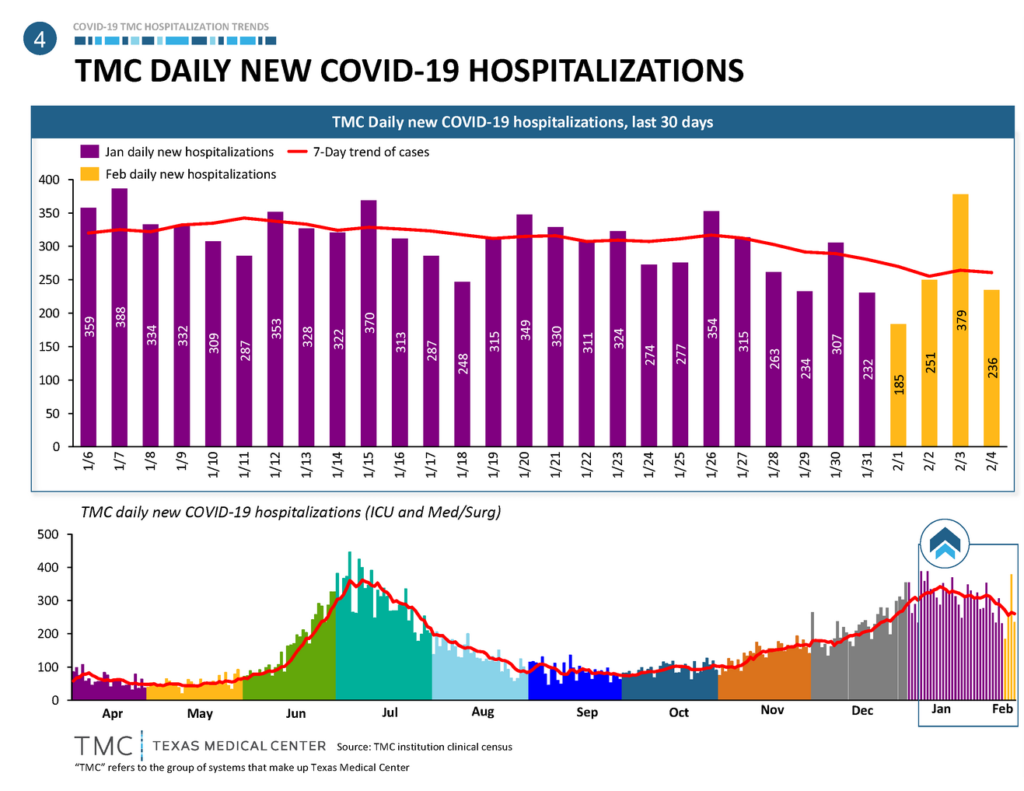
Although the hospitalization rate in Houston is still high, it’s pretty clear now that we passed a peak and it’s going down. This means my predictions were, fortunately, wrong.
The daily new positive cases are still pretty high.
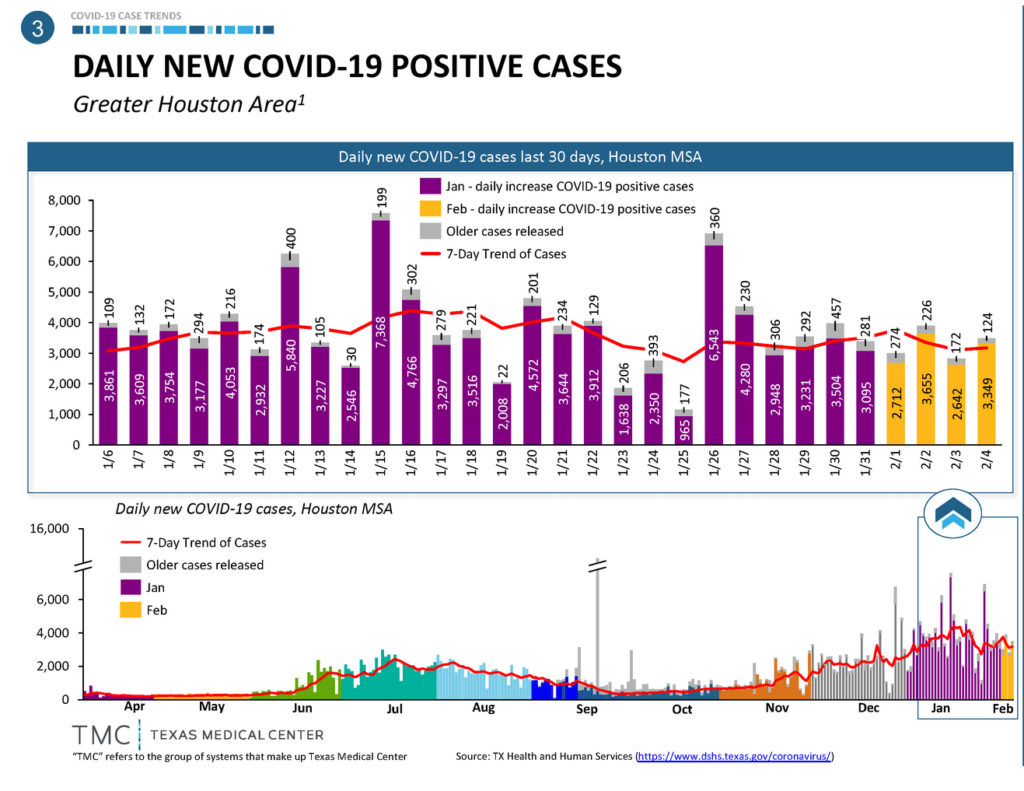
What’s going on here? I wish I could tell you that people are being more careful, but my small, careful outings into the community reinforce my bleak view of human nature. We, as a whole, are not being particularly careful.
As a refresher, why do I care about/harp on hospitalizations so much? For two reasons: The first is because they are predictive of deaths, so less hospitalizations means less people will die. The second is because, after a threshold, they have compounding bad effects. If the hospitals get saturated enough, people die of milder cases because they can’t get help, and people with other conditions die as well. And the healthcare personnel get sick and/or burn out, further compounding the problem
What IS going on, then? It’s a combination of things. I credit two factors. Both of them are, or would be (if I got it right), genuinely good news.
Factor one, and this one isn’t a guess: we are relentlessly getting better at figuring out who is in danger of immediate serious complications* or not, and admitting people who truly need it to the hospital, letting milder cases play out at home.
Factor two, an educated guess: the vaccines are having an effect already. The vaccination strategy is fractured and frustrating, leaving people who want them scrambling for shots. However, the vaccines do work, and we’ve -haphazardly, but correctly- prioritized the most vulnerable, and the healthcare personnel who are both necessary, and at risk of being vectors. Aside: under the same logic, please vaccinate the teachers NOW.
As of this writing, 11 doses of vaccine per 100 people have been distributed in the US. This doesn’t mean 11% of people are fully vaccinated, because the vaccines require two doses. Most people have one shot in them, which confers some protection, and a few already have both.
In Harris County, approximately 9% of the eligible population already has received one shot (click on the image below to access an interactive dashboard). If this was a randomly-distributed 9% of the population, the impact would be minimal; but it’s a selected group of vulnerable individuals, with the most likelihood of getting very sick or dying. This likely makes a big difference in hospitalization rates, so I expect them to continue falling.
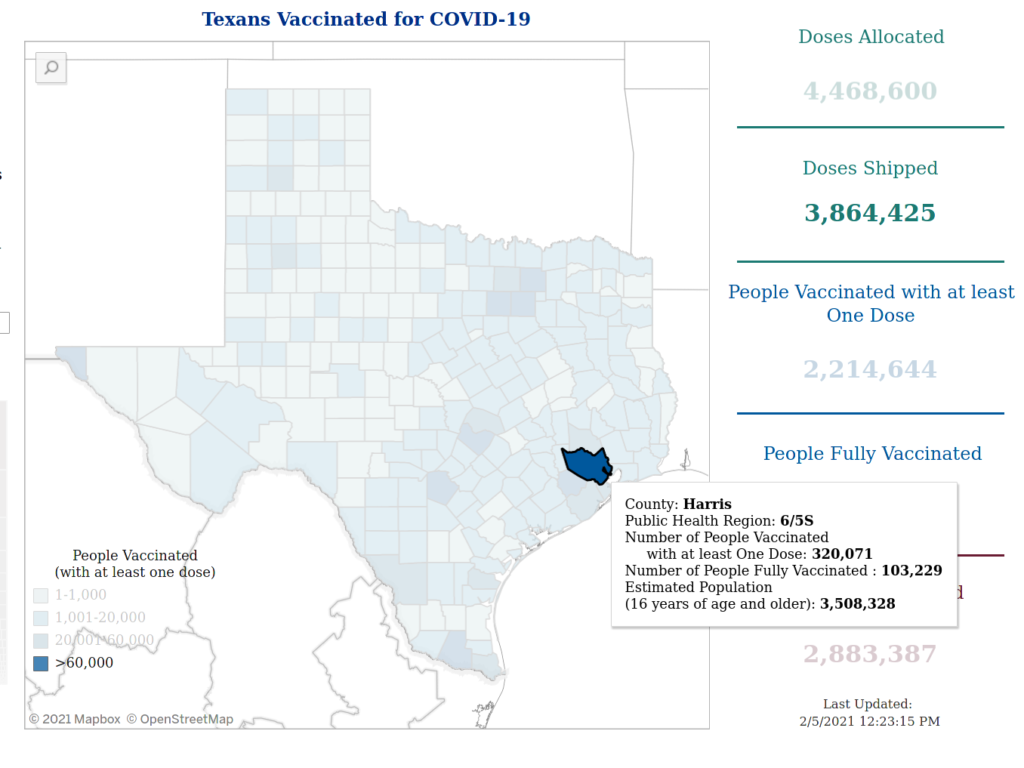
(Note that the doses allocated/shipped above are for all of Texas, and the Harris County data is in the small popup)
The strategy of allocating vaccines to vulnerable people first poses an ethical question, which is should I get one if I’m not at immediate risk but somehow get on a list? I agree with this NY Times opinion piece: get it. On one hand, gauging your own risk is not that easy. On the other, getting more people vaccinated is a net good. On the gripping hand, there are no guarantees it’ll go to someone who needs it more than you do. Barring genuine counter-indications, we should all get vaccinated if at all possible. You’re arguing timing in marginalia.
Finally, I leave you with a counterargument to one of the dumbest antivaxx conspiracy theories.

*By “immediate serious complications” I mean things that will kill you quickly. All available evidence on long-term complications (“long-haul COVID”) shows that they can be very, very bad, and we have -so far- no way of knowing who’ll have or not. If you prance about the community without a mask on and act carelessly, thinking the doctors will save you if necessary, you’re a selfish dumbass.